
HIV SURVEILLANCE AND RESPONSE
HIV surveillance is underway in the district, and there is important learning about HIV surveillance from the effort, as well as achievements that have resulted from the process. The pilot use of Integrated Disease Surveillance and Response (IDSR) approaches for HIV (IDSR-HIV pilot) has been successful in strengthening the capacity at community and district levels, integrating passive and active surveillance of HIV risk and infections into the normal business practice of the district’s HIV prevention efforts, and engaged communities in surveillance, detection, and response.
Importantly, the District has grown in its technical leadership and governance of HIV surveillance and response efforts. There is coordination happening around risk signals, existing hotspots, and response actions where there was none at the start of BPS. People in the community are cognizant of HIV risks, and there is shared language about issues and response activities. As a result, there is greater coherence and coordination of resources for HIV prevention across the district. Community Health Team participation in identifying risks and responding to the HIV epidemic in Blantyre is resulting in more effective and targeted public health interventions.
Elements of Blantyre’s HIV surveillance and response approach include:
Use of a common data platform (PALMS) is a core element of Blantyre’s integrated HIV surveillance system. It allows for transparency across district and city health teams, facilities, partners, and others about areas of concern and enables quick identification of problem areas through its color-coded flags.
Capacitated human resources at district, facility, and community levels – In addition to having PALMS as a common platform, the capacities that have been built through BPS support such as governance and technical leadership, data access and use, and surveillance and response approaches are integral to enabling active and passive surveillance.
Passive Surveillance in Blantyre involves the systematic identification, collection, monitoring, analysis, and interpretation of structured data. It is conducted primarily at facilities; however, the district and city health teams, network model committees, and others review data routinely to identify issues and opportunities for response. Blantyre’s passive surveillance leverages the PALMS platform including monitoring of 13 defined indicators (diagnostic and risk). The thresholds for what triggers an investigation or response are included in the defined green, yellow, and red flags for each indicator in PALMS.
Active Surveillance in Blantyre is primarily community-based with signal reporting from key informants up to facilities and to the district health team. Blantyre’s approach to active surveillance has included responding to signals from known hotspots as well as event-based surveillance defined as the organized and rapid capture of information about events that are of potential HIV infection risk to public health. In addition to passive surveillance and active support in known hotspots, the District health team has trained Health Surveillance Assistants (HSAs), Community Health Team (CHT) members, and other community health workers to identify risk signals and support necessary and timely interventions. CHTs are often the first line of contact between communities and the health system and are well placed to provide critical insight into high-risk communities to inform where HIV prevention interventions should be targeted. In addition, in the CY 2024 Quarter 2, the District Environmental Health Office began training “surveillance informants”, i.e. CHTs and other community health structures and key informants (e.g. shop owners, village leaders, and schoolteachers) how to capture data about events in the 11 catchment areas.
Lessons learned:
-
Use of a common data platform has been critical to rolling out and supporting HIV surveillance and response activities and the coordination between district, facility, and community.
-
Access to data is critical but insufficient on its own. Health workers need training in data interpretation and analysis to support their decision making, including understanding indicators and triangulation.
-
Capacitation cannot stop at the Environmental Health Office at district or facility level. To support active and passive surveillance, capacitating other district coordinators, health facility staff, community health teams, and community members is valuable. It creates a collaborative mentality and improves coordination during response efforts.
-
The indicators developed in the first phase of implementation need to be revisited based on experience. A working group with local and global experts will be established to support the review and revision process.
-
There is opportunity for a community of practice among facilities to learn about common signals and effective responses.
Two illustrative case studies (below) demonstrate how health workers are using data and related signals or “flags” in PALMS as passive surveillance to spur investigation and response. While these are case studies and absolute causality is not possible, they are two of many such examples that highlight how local data use is driving HIV prevention activity that would not have been possible without data visualization and use.
In case study #1, health workers noted low PrEP uptake (identified through PALMS) among students attending a local college (MUBAS) (see Figure 2). Three non-sequential actions were taken to try to understand and address the issue. The first was a July 2023 community lab, which gathered insights that identified unique gaps on PrEP knowledge, concerns about accessibility, and use among students; and misuse of PrEP including sharing pill bottles. A second action was taken at facility level. The insights from the community lab informed QI change ideas at Gateway Clinic, e.g. changing location of the PrEP room and intensifying screening and education at all entry points. The third action was taken at community level to reach the students directly. A health promotion and service delivery event was held in February 2024 in the community at the campus under the BPS Konda Blantyre, Konda Moyo (Love Blantyre, Love Life campaign). During the event, the network model committee worked together to distribute condoms and HIV self-testing kits and share information for HIV services and products within the catchment area of the university.

Figure 2. Use of passive surveillance informs additional action for MUBAS students
Following investigation/programmatic action, there was a subsequent rise in HIV testing, PrEP use, and decreased new HIV infections diagnosed at/around the local clinic (Gateway) serving the students (see Figure 4). The number assessed for PrEP stayed relatively constant for the subsequent quarter. The immediate increase in new initiations spiked to more than 60 in the quarter with the network campaign event but levelled off to just over 40 in quarters 3-4 of 2024 (see Figure 5). There was a noted decrease in 2025 quarter 1 likely due to the USG SOW.

Figure 4. Increased testing and PrEP initiation at Gateway Clinic
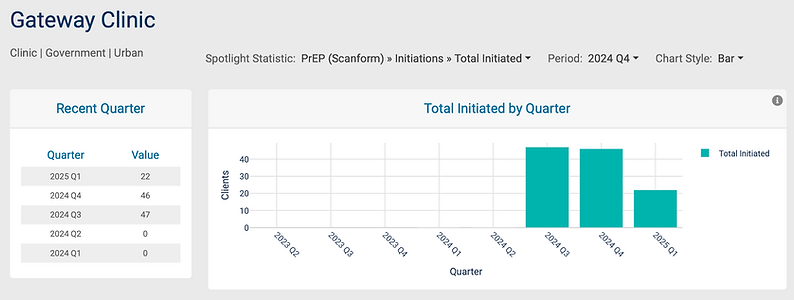
Figure 5. Continuing PrEP initiation at Gateway Clinic (source: PALMS, accessed May 30, 2025)
A second illustrative case study of passive surveillance leading to investigation and response comes from Kadidi (Figure 6). Health workers at Kadidi health centre used PALMS during a data review meeting and noted an increase in HIV infections. While investigating, the health workers on the FRRT discovered new hotspots. They worked with the network model committee for the Kadidi catchment area to organize activities in the community to address the risk issues. There was a subsequent decrease in HIV positivity at Kadidi following implementation of the activities (Figure 7).

Figure 6. Passive surveillance, investigation, and response at Kadidi Health Center

Figure 7. Decrease in HIV positivity at Kadidi Health Center
